Adductor Brevis
- Fysiobasen

- Jan 11
- 8 min read
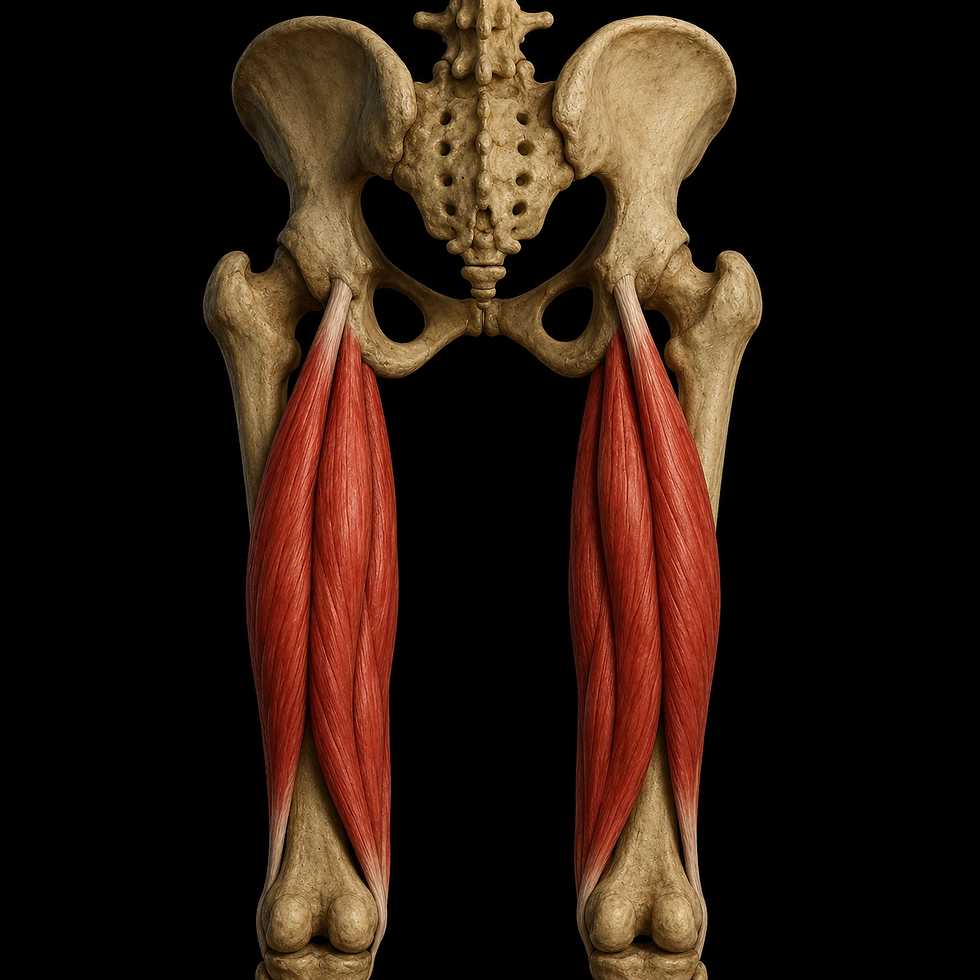
The adductor brevis is a short, fan-shaped muscle of the medial thigh and belongs to the adductor muscle group. It is located deep to the pectineus and adductor longus, and anterior to the adductor magnus. Although smaller in size compared with its neighbouring muscles, it plays an important role in hip function, particularly during gait and pelvic stabilisation. The adductor brevis also contributes to fine adjustment of hip joint movements, which is essential during rapid changes of direction and balance in standing.

Origin
Body of the pubic bone (anterior part of the pubis)
Inferior pubic ramus (lower branch of the pubic bone)
The muscle has a narrow but clearly defined origin from the anterior surface of the pubis and the lateral portion of the inferior pubic ramus. The origin lies deep and close to the pubic symphysis and marks the beginning of muscle fibres that spread in a fan-like pattern laterally and inferiorly toward the femur. This origin provides a favourable mechanical lever for adduction and rotation, particularly during light, rapid movements requiring controlled activation.
Insertion
Medial lip of the linea aspera of the femur (upper half)
The muscle inserts broadly along the medial lip of the linea aspera on the posterior aspect of the femur. The insertion extends over the upper third of the femoral shaft and is located between the pectineus (more proximal and medial) and the adductor magnus (more distal and lateral). In addition to its primary aponeurotic attachment to the linea aspera, some fibres may blend with adjacent musculature, creating a functional transition between different components of the adductor group.
This insertion gives the adductor brevis favourable conditions for both force production and precision of movement. Its anatomical position also allows controlled movement under varying loads, which is central in sports and dynamic activities.
Relations to Adjacent Structures
Anatomically, the adductor brevis functions as a central element within the adductor group. It is located:
Deep to: the pectineus and adductor longus
Superficial to: the adductor magnus and obturator externus
Closely related to: the obturator nerve, which divides into an anterior and posterior branch on either side of the muscle
Inferiorly: in contact with the gracilis muscle on the medial thigh
This position makes the adductor brevis an important landmark during dissection and surgical procedures in the groin and pelvic region. Its relationship to the perforating arteries and the obturator nerve also makes it vulnerable during certain injuries and interventions.
Innervation
The adductor brevis is innervated by the obturator nerve (L2–L4), which arises from the anterior division of the lumbar plexus. The nerve passes through the obturator canal and divides into two branches that surround the muscle—one anterior and one posterior.
This branching pattern gives the adductor brevis a characteristic topographical relationship that can be used clinically during neurological assessment. The nerve supply enables rapid contraction and fine motor control, which are essential for balance and directional changes.
Blood Supply
The primary blood supply to the adductor brevis is provided by the profunda femoris artery, which gives off perforating branches to the adductor group. In addition, contributions come from:
The obturator artery, via its proximal branches
The medial circumflex femoral artery, through collateral connections
These vessels form a rich anastomotic network around the muscle, ensuring adequate oxygen delivery even during prolonged or repetitive activity. The generous blood supply is also advantageous for recovery following microtrauma and in the management of tendinopathies.
Function
The primary function of the adductor brevis is adduction of the thigh, drawing the femur toward the body’s midline. In addition, it contributes to:
Hip flexion, particularly in neutral or slightly flexed positions
Rotation: Due to its anatomical position, the muscle may assist in both internal and external rotation depending on hip joint position and the specific fibres activated
Pelvic stabilisation: During gait, especially in single-leg stance, the muscle helps maintain a level pelvis by drawing toward the stance limb
The adductor group, including the adductor brevis, is highly active in closed kinetic chain activities such as standing, walking, running, and kicking. The brevis functions both dynamically and isometrically to control movements in the frontal plane and reduce load on ligaments and the joint capsule.
Clinical Significance of the Adductor Brevis
The adductor brevis plays a subtle yet critical role in hip joint biomechanics. Weakness or injury rarely leads to complete functional loss but may disrupt fine motor control and load distribution within the hip–pelvis–knee chain. This is particularly noticeable during rotation, rapid directional changes, or overload in sports requiring hip stability and agility.
With unilateral weakness, compensatory patterns may develop, including overuse of the tensor fasciae latae or iliopsoas and increased medial loading at the knee. This increases the risk of secondary conditions such as medial knee pain, trochanteric tendinopathies, or non-specific groin pain.
Adductor-Related Injuries
One of the most common clinical conditions involving the adductor brevis is adductor tendinopathy, particularly affecting athletes in sports such as:
Football (soccer)
Ice hockey
Handball
Martial arts
Long-distance running
Adductor tendinopathy is characterised by gradually developing groin pain, often most pronounced during passive abduction or active adduction. The most common injury component is overload of the tendon attachment at the pubis, where the adductor brevis also attaches. The brevis is more frequently involved than previously assumed, particularly in long-standing cases with poor response to rehabilitation targeting only the adductor longus.
Risk factors include previous groin injury, weak core musculature, reduced hip flexor mobility, and imbalance between adductors and abductors. Anatomical variations such as leg length discrepancy or increased foot pronation may also contribute.
Trigger Points and Referred Pain
The adductor brevis has documented myofascial trigger points that commonly produce referred pain:
Into the groin
Down the medial thigh
In some cases toward the medial aspect of the knee
These trigger points are often difficult to palpate in isolation due to the muscle’s deep location and are easily mistaken for pain originating from the adductor longus or gracilis. In cases of persistent groin pain that do not improve with standard adductor training, the adductor brevis should be considered as a potential source.
Biomechanical Role in Gait and Sport
During walking and running, the adductor brevis is activated isometrically during the stance phase to prevent excessive lateral pelvic movement. In addition, during early push-off it contributes to rapidly drawing the thigh toward the midline, with a combined moment of flexion and rotation. This role is particularly important in sports that require lateral acceleration and rapid changes of direction.
In the frontal plane, the adductor brevis stabilises the hip by counteracting abduction forces. In the transverse plane, it fine-tunes internal and external rotation in cooperation with the deeper layers of the adductor muscle group.
With weakness or inhibition of the adductor brevis (for example following injury), the following may be observed:
Increased lateral collapse of the knee (valgus alignment)
Reduced control during single-leg exercises
Increased risk of adductor injury on the contralateral side due to asymmetry
Examination and Testing
Palpation of the adductor brevis requires precision and knowledge of surrounding structures. The muscle lies deep within the groin and requires the patient to be positioned in slight external rotation and mild hip flexion for optimal access. Direct palpation toward the medial aspect of the femur, proximally and deep to the adductor longus, provides the most accurate localisation.
There are no isolated specific tests for the adductor brevis, but the following assessments may provide useful clinical information:
Adductor squeeze test:The patient squeezes the knees together against resistance at varying joint angles (0°, 45°, 90°). Pain at lower angles may indicate brevis involvement.
Resisted adduction test:Performed in supine with the hip in slight flexion and the knee extended. Resistance against adduction in this position strongly activates the adductor brevis.
Stretch test with abduction and external rotation:Pain in this position often implicates the adductor brevis, as the muscle is maximally stretched here.
In cases of suspected chronic dysfunction, dynamic testing is also recommended, including single-leg squat and step-down tests, to assess hip control during functional movement.
Principles of Rehabilitation for the Adductor Brevis
Injury to the adductor brevis—whether as part of a tendinopathy, muscle strain, or postural overload—requires restoration of controlled force production, tissue tolerance, and functional symmetry of the hip joint and pelvis. Rehabilitation must be individualised based on whether the condition is acute or chronic, and whether symptoms are local or referred via surrounding structures.
A common clinical error is excessive focus on stretching and unloading alone. In long-standing adductor-related pain, current evidence shows that progressive strength training produces superior and more durable outcomes compared with passive interventions alone¹. This also applies to the adductor brevis, despite its smaller size and deeper location.
Phase-Based Rehabilitation Approach
1. Acute Phase (0–5 days)
The goal is to reduce pain and protect against further injury. Provocative movements should be avoided, especially rapid abduction or unexpected stretching.
Interventions:
Relative rest with controlled movement
Ice and light compression
Gentle activation of surrounding musculature without pain
2. Early Rehabilitation Phase (5–14 days)
The goal is to restore controlled contraction of the adductors, with emphasis on reactive activation of the adductor brevis.
Interventions:
Isometric adduction with knees flexed at 30–60°
Balance exercises in standing with controlled weight-bearing
Light sling-based exercises and nerve flossing if obturator nerve irritation is present
3. Progressive Strength Phase (2–6 weeks)
Load is gradually increased, with emphasis on eccentric control and movements in which the adductor brevis is particularly active.
Interventions:
Copenhagen adduction exercises at low and high angles
Slideboard adduction (sliding movements from standing)
Dynamic squats with elastic resistance in the frontal plane for medial stabilisation
Lunge training with added hip rotation
4. Return to Sport (from week 6)
Full strength and control should be tested under maximal directional changes and high-speed frontal plane movements.
Interventions:
Running drills with lateral changes of direction
Lateral bounding and skating jumps
High-speed adduction exercises with eccentric braking phases
Sport-specific drills with progressively increasing intensity
Targeted Exercises for the Adductor Brevis
1. Isometric Knee Squeeze With Ball
Execution: The patient lies supine with hips and knees flexed to 90°. A soft ball is placed between the knees. The patient squeezes for 5–10 seconds, repeated 10–12 times.
Effect: Activates the adductor brevis at a controlled joint angle. Suitable for early-stage rehabilitation without provoking pain.
2. Modified Copenhagen Adduction Lift
Execution: The patient lies on the side with the lower limb supported on a bench and the upper body supported by the arms. The upper leg is slowly lifted and lowered.
Effect: Highly effective for the adductor brevis in addition to the adductor longus. Begin with bent knees and progress gradually to full extension.
3. Sliding Adduction on Towel
Execution: The patient stands with one foot on the floor and the other on a towel or slider. The sliding leg moves out to the side and is then drawn back slowly with controlled activation.
Effect: Provides eccentric loading of the entire adductor group. Difficulty can be adjusted via friction and movement speed.
4. Single-Leg Squat With Emphasis on Medial Stability
Execution: The patient performs slow single-leg squats. An elastic band pulls laterally at pelvic height to challenge the hip adductors.
Effect: Stimulates the adductor brevis through isometric medial support and transverse-plane control.
Physiotherapeutic Follow-Up
In cases of persistent symptoms, it is essential to assess:
Hip rotational control
Lumbopelvic rhythm
Foot posture and pronation pattern
Asymmetrical loading during standing and gait
A structured approach combining manual assessment, functional testing, and strength measurement is necessary to ensure appropriate intervention at the right stage. Many patients with adductor brevis pathology respond best to a multidisciplinary strategy, including guided exercise, training load modification, and screening for biomechanical deviations in the lower extremity.
Concluding Remarks
The adductor brevis is a small but clinically significant muscle that is often overlooked in groin-related conditions. With thorough assessment, targeted rehabilitation, and appropriately dosed strength training, full recovery and functional return can be achieved—even in highly active athletes. Understanding the muscle’s anatomy, function, and clinical relevance provides the physiotherapist with a clear advantage in managing disorders of the hip–groin complex.
References
Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2014). Clinically Oriented Anatomy (7th ed.). Lippincott Williams & Wilkins.
Palastanga, N., & Soames, R. (2012). Anatomy and Human Movement: Structure and Function (6th ed.). Churchill Livingstone.
Standring, S. (2016). Gray’s Anatomy (41st ed.). Elsevier Churchill Livingstone.
Netter, F. (2014). Atlas of Human Anatomy (6th ed.). Saunders.