

Gluteus Maximus
- Fysiobasen

- Apr 14
- 10 min read
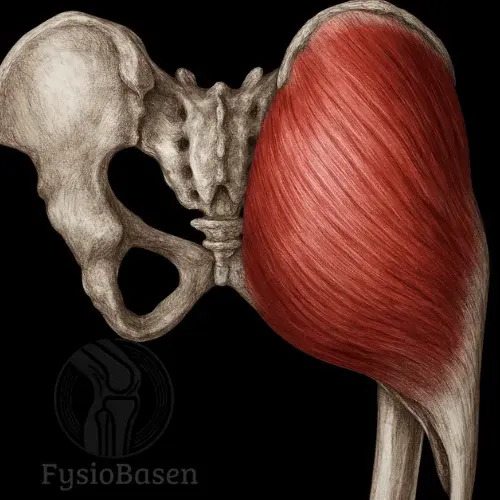
Gluteus maximus is the body’s largest and most superficial muscle, and it makes up the main bulk of the gluteal region. It plays a central role in functions such as upright posture, walking, running, and rising from a seated position. Gluteus maximus is a powerful hip extensor and an important stabilizer of the pelvis. Its anatomical location and influence on the hip and lumbar region make it a critical focus in both rehabilitation and performance-
oriented training.
Main points
Gluteus maximus – key anatomical points
Topic | Key point |
Muscle type | The largest and most superficial gluteal muscle in the body |
Location | Forms the main bulk of the gluteal region |
Origin | Ilium posterior to the posterior gluteal line, sacrum, coccyx, sacrotuberous ligament, and thoracolumbar fascia |
Insertion | Iliotibial tract and gluteal tuberosity of the femur |
Fiber direction | Obliquely lateral and downward |
Layering | Superficial fibers insert into the iliotibial tract, deep fibers into the femur |
Innervation | Inferior gluteal nerve, L5–S2 |
Blood supply | Inferior gluteal artery and partly the superior gluteal artery |
Gluteus maximus – function and biomechanics
Topic | Key point |
Primary function | Hip extension |
Secondary functions | External rotation, contribution to abduction and adduction depending on fiber direction |
Postural role | Stabilizes the pelvis and helps control lumbar lordosis |
Walking | Activated especially during late stance to support hip extension and pelvic control |
Running and sprinting | Important for propulsion, force production, and stability |
Eccentric role | Decelerates hip flexion and controls loading during landing and descending |
Lumbopelvic control | Works together with the thoracolumbar fascia, hamstrings, transversus abdominis, and pelvic floor |
Gluteus maximus – anatomical relations and clinical relevance
Topic | Key point |
Structures it covers | Gluteus medius, ischial tuberosity, sciatic nerve, ischial and trochanteric bursae |
Structures it influences | Thoracolumbar fascia, sacrotuberous ligament, posterior gluteal line, and dorsal ilium |
Common consequences of weakness | Lumbar low back pain, reduced hip extension, poor pelvic control |
Compensations | Overactivity of the hamstrings and hip flexors |
Postural changes | Anterior pelvic tilt and increased lordosis |
Functional signs | Weakness during stair climbing, running, and rising from a chair |
Possible overload issues | Gluteal bursitis and local irritation during prolonged sitting |
Palpation, examination, and findings
Topic | Key point |
Palpation position | Prone with the hip in neutral |
Palpation direction | Obliquely from the ilium and sacrum toward the femur |
Activation test | The patient lifts the thigh off the surface against resistance |
What to assess | Muscle activation, force production, pain, side-to-side difference, and compensation |
Clinical observation | Use of the arms when rising may indicate gluteus maximus weakness |
Differential consideration | Local gluteal pain may be mistaken for sciatica if symptoms radiate |
Most effective exercises for gluteus maximus
Exercise | Main benefit | Typical use |
Hip thrust | Very high gluteal activation and strong peak contraction | Hypertrophy, maximal strength, power |
Deep squat | High activation with large hip flexion | Functional strength, explosiveness |
Bulgarian split squat | High unilateral loading and stability demand | Sport, injury prevention, rehab |
High box step-up | Strong activation early in the movement | Walking, running, functional training |
Glute bridge | Safe and effective activation with lower demands | Warm-up, pre-activation, rehabilitation |
Romanian deadlift | Strong eccentric loading together with the hamstrings | Sprinting, jumping, posterior chain |
Origin
Gluteus maximus has a broad and complex origin that includes both bony and ligamentous structures:
• Ilium, posterior to the posterior gluteal line (linea glutea posterior)
• Sacrum, dorsal surface
• Coccyx
• Sacrotuberous ligament
• Thoracolumbar fascia
This broad origin reflects the muscle’s function as a force producer and postural supporter, and helps explain why it is active in so many movements involving the hip joint and pelvis.
Insertion
Gluteus maximus has two main insertions that emphasize its role in both mobility and stability:
• Iliotibial tract, upper lateral part of the muscle
• Gluteal tuberosity of the femur, deeper and more medial fibers
This two-part insertion arrangement means that gluteus maximus affects both the hip and knee joints through its connection to the iliotibial tract. It also provides a mechanical basis for combining force production with controlled movement.
Topographic Location and Structure
Gluteus maximus covers the underlying muscles of the gluteal region, including gluteus medius, gluteus minimus, and several small external rotators, such as piriformis, gemelli, and obturator internus. The muscle is clearly visible and palpable, and its volume varies greatly depending on training status, genetics, and function.
The fibers are oriented obliquely laterally and downward, running from the broad bony origin to the narrower and deeper insertions. The muscle is divided into superficial and deep fibers, where the superficial fibers mainly insert into the iliotibial tract and the deep fibers into the femur.
Function and Movement
Gluteus maximus is the primary extensor of the hip joint. This means that it is mainly responsible for moving the thigh backward, a movement called hip extension. This function is essential for basic movements such as standing up from a chair, climbing stairs, running, and jumping.
• Hip extension: Activated especially when the hip must be extended from a flexed position, for example when rising from sitting or during the push-off phase of running.
• External rotation of the hip joint: When it contracts, gluteus maximus pulls the femur outward, meaning lateral rotation, a movement that is important for stability and power during rapid changes of direction.
• Abduction and adduction: The upper fibers contribute to abduction, moving the leg away from the midline, while the lower fibers can assist in adduction, moving the leg toward the midline, depending on position and direction of movement.
• Extension of the pelvis on the femur: With the femur fixed, in standing, gluteus maximus tilts the pelvis backward and reduces lumbar lordosis. This is especially important for postural control in standing and during heavy loading.
Gluteus maximus often works eccentrically, meaning that it slows movement, especially during descending stairs, landing, or hip flexion under controlled load. This provides stability and braking force in dynamic situations.
Biomechanical Role in Walking and Running
During walking, gluteus maximus is activated particularly in the late stance phase, just before the foot leaves the ground. It then contributes to hip extension while also stabilizing the pelvis and preventing anterior tilt.
During running and sprinting, the load on gluteus maximus increases significantly, and it is strongly activated to generate forward propulsion and maintain pelvic control. Reduced activation or weakness in this muscle can lead to compensatory patterns in the hamstrings, lumbar spine, or opposite hip.
Postural Stabilization and Lumbopelvic Control
Gluteus maximus has a central function in the lumbopelvic complex, the area where the lower back, pelvis, and hip meet. Together with the thoracolumbar fascia, hamstrings, transversus abdominis, and pelvic floor musculature, gluteus maximus is part of an interaction that controls movement and stability in this region.
Its contribution to keeping the pelvis in a neutral position is important in both standing and dynamic situations. With weakness or delayed activation, anterior pelvic tilt, increased lordosis, and instability often occur, which in turn can lead to pain in the lower back, hip, or knee.
Synergists and Antagonistic Balance
• Synergists: The hamstrings, biceps femoris, semitendinosus, and semimembranosus, assist in hip extension, but have a smaller moment arm in extreme positions. Adductor magnus, posterior part, also functions as a powerful extensor at certain angles.
• Antagonists: Iliopsoas and rectus femoris oppose gluteus maximus during hip extension. With overactivity in these muscles, for example from prolonged sitting, gluteus maximus may be inhibited through neuromuscular reflex pathways, known as “gluteal amnesia.”
To achieve optimal function and injury prevention, good balance and coordination between these muscle groups are required. In clinical practice, it is common to see underactive gluteal muscles, which should be addressed with specific exercises and conscious activation.
Innervation
Gluteus maximus is innervated by the inferior gluteal nerve, which is a motor nerve formed by the spinal segments L5, S1, and S2. This is an important nerve branch from the sacral plexus.
• Nerve pathway: The nerve leaves the pelvis through the lower part of the greater sciatic foramen, below the piriformis muscle.
• Course: After passing out of the pelvis, it runs deep to gluteus maximus and branches into many small motor nerves that go to different parts of the muscle.
Clinical relevance:
• In the event of injury or compression of the inferior gluteal nerve, reduced ability to extend the hip may be seen, especially in functional movements such as stair climbing and lifting.
• The nerve is tested indirectly through strength testing and functional movement analysis.
Blood Supply
Gluteus maximus has a rich blood supply system to support its powerful and enduring function.
Main Arteries
• Inferior gluteal artery, primary blood supply
• Superior gluteal artery, partly supplies the upper parts of the muscle
These arteries arise from the internal iliac artery and follow the same course as the inferior gluteal nerve through the greater sciatic foramen.
Venous Drainage
• The inferior and superior gluteal veins follow the corresponding arteries and drain into the internal pelvic venous system.
Good circulation in the area is important for recovery and tissue health.
Anatomical Relations
Gluteus maximus is a superficial and powerful muscle that covers several deep structures.
Structures it covers:
• Gluteus medius, almost entirely
• Ischial tuberosity, when the hip is extended
• Sciatic nerve, the largest peripheral nerve in the body, which passes deep to gluteus maximus
• Ischial and trochanteric bursae, synovial bursae that reduce friction between muscle and bone
Structures it is attached to or influences:
• Thoracolumbar fascia
• Sacrotuberous ligament
• Posterior gluteal line and dorsal ilium
Clinical Significance
Gluteus maximus is involved in a number of clinical presentations and dysfunctions. Reduced activation or muscle strength is associated with:
• Lumbar low back pain, often secondary to weakness in hip extension and reduced lumbopelvic control
• Overcompensation by the hamstrings, which can lead to tendinopathies and posterior thigh symptoms
• Anterior pelvic tilt and increased lordosis, with reduced tone in the gluteal muscles and overactivity in the hip flexors
• Weakness during stair climbing and rising, where gluteus maximus weakness may be revealed when patients need to use their arms to rise from a chair
Palpation and Examination
Palpation of gluteus maximus is best performed with the patient in the prone position and the hip in a neutral position. The muscle is palpated obliquely from the ilium and sacrum toward the femur. Activation can be tested by asking the patient to lift the thigh off the surface against resistance.
Bursitis and Overuse-Related Complaints
With prolonged sitting or repetitive movements, friction may develop over the ischial tuberosity, which can lead to gluteal bursitis. This causes local pain and may be mistaken for sciatica if the pain radiates.
Gluteus Maximus – The Most Effective Exercises
Gluteus maximus is the body’s largest and most powerful muscle, and a central contributor to hip extension, upright posture, walking, and explosive movement. For optimal training of this muscle, the exercises must challenge hip flexion and create high mechanical tension in the extension phase.
Research shows that the most effective exercises are those that:
• Involve large hip flexion, more than 90 degrees
• Have external resistance in a horizontal direction, such as the hip thrust
• Or vertical loading, such as the squat, with a deep range of motion
• Activate the gluteus with high EMG activity, more than 70 percent of maximum
1. Hip Thrust
Effect: Extremely high activation of gluteus maximus, especially in the top position where hip extension is greatest.
Explanation: The hip thrust isolates the gluteal musculature with little assistance from the hamstrings or quadriceps. The exercise loads the hip horizontally, and research shows that this provides more specific activation of the gluteus than vertical exercises.
Research: A study by Contreras et al. (2015) showed that the hip thrust reached more than 100 percent of maximal EMG contraction in gluteus maximus, more than both the squat and the deadlift at similar relative loads.
Particularly effective for:
• Gluteal hypertrophy
• Maximal strength development in hip extension
• Stabilization during jumping and running
2. Deep Squats
Effect: High activation of gluteus maximus when the hip goes below 90 degrees.
Explanation: Squats activate the entire lower extremity. The deeper you go, the more stretch occurs in the gluteus, which leads to greater force development in the concentric phase. Squats are also functional, with good transfer to everyday and athletic movements.
Research: EMG analyses show that depth has a major influence on gluteal activation. Gluteal activation in parallel squats is approximately 40 percent lower than in deep squats.⁴
Particularly effective for:
• Functional strength and explosiveness
• Coordination and core stability
• Overall leg strength, with high transfer value
3. Bulgarian Split Squat
Effect: Combines high gluteal activation with demands on stability and unilateral control.
Explanation: The rear foot is placed on a bench, and the front leg performs a squat-like movement. The exercise provides a large hip range of motion and requires the gluteus to decelerate and drive the movement alone, without support from the opposite leg.
Research: Studies have shown that the Bulgarian split squat produces higher gluteal activation than the regular lunge, especially in the eccentric phase.⁵
Particularly effective for:
• Sport-specific strength and balance
• Rehabilitation and injury prevention
• Gluteus-dominant unilateral strength
4. Step-Up onto a High Box
Effect: Gluteus maximus performs substantial work in the initial phase because of the large hip angle.
Explanation: By using a high box, at least knee height, you achieve significant hip flexion and force the gluteus to drive the movement. It is crucial not to “push” with the back leg.
Research: A comparison of gluteal activation showed that step-ups with 90 degrees of hip flexion produce EMG levels comparable to the hip thrust.⁶
Particularly effective for:
• Functional strength in walking and running
• Gluteal activation in the early movement phase
• Rehabilitation after hip or pelvic injury
5. Glute Bridge, With or Without Weight
Effect: Moderate to high activation, depending on load and execution.
Explanation: It resembles the hip thrust, but the range of motion is smaller. For beginners and patients with pain, it is a safe and effective way to begin activation.
Research: According to a study by Boren et al. (2011), the single-leg glute bridge provides approximately 80 percent of maximal gluteal activity, which makes it highly useful in clinical settings.⁷
Particularly effective for:
• Rehabilitation, pre-activation, and warm-up
• Isolated activation
• Individuals with limited mobility in the knee or back
6. Romanian Deadlift, RDL
Effect: Activates the gluteus effectively together with the hamstrings, especially in the eccentric phase.
Explanation: Although the RDL does not isolate the gluteus, it helps develop hip extension under stretch, which builds eccentric control and strength.
Research: Studies show that the RDL produces moderate to high activation of the gluteus, but lower than the hip thrust and squat. Even so, it remains valuable because of its functional transfer.⁸
Particularly effective for:
• Hamstrings and gluteus working together
• Eccentric strength for sprinting and jumping
• Counteracting hamstring dominance
Conclusion – What Does the Research Say?
• Hip thrust is best for pure activation and isolation
• Deep squats and Bulgarian split squats provide the best functional transfer
• The glute bridge is best for beginners, rehabilitation, and pre-activation
• Step-ups and RDLs complement training with functional and eccentric elements
By combining these exercises, you gain:
• Maximal EMG activation
• Varied loading directions
• Transferability to sport and daily movement
Sources
Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2014). Clinically Oriented Anatomy (7th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Palastanga, N., & Soames, R. (2012). Anatomy and Human Movement: Structure and Function (6th ed.). Edinburgh: Churchill Livingstone.
Standring, S. (2016). Gray’s Anatomy (41st ed.). Edinburgh: Elsevier Churchill Livingstone.
Netter, F. (2014). Atlas of Human Anatomy (6th ed.). Philadelphia, PA: Saunders.



