Hamstrings
- Fysiobasen

- Jun 3
- 14 min read
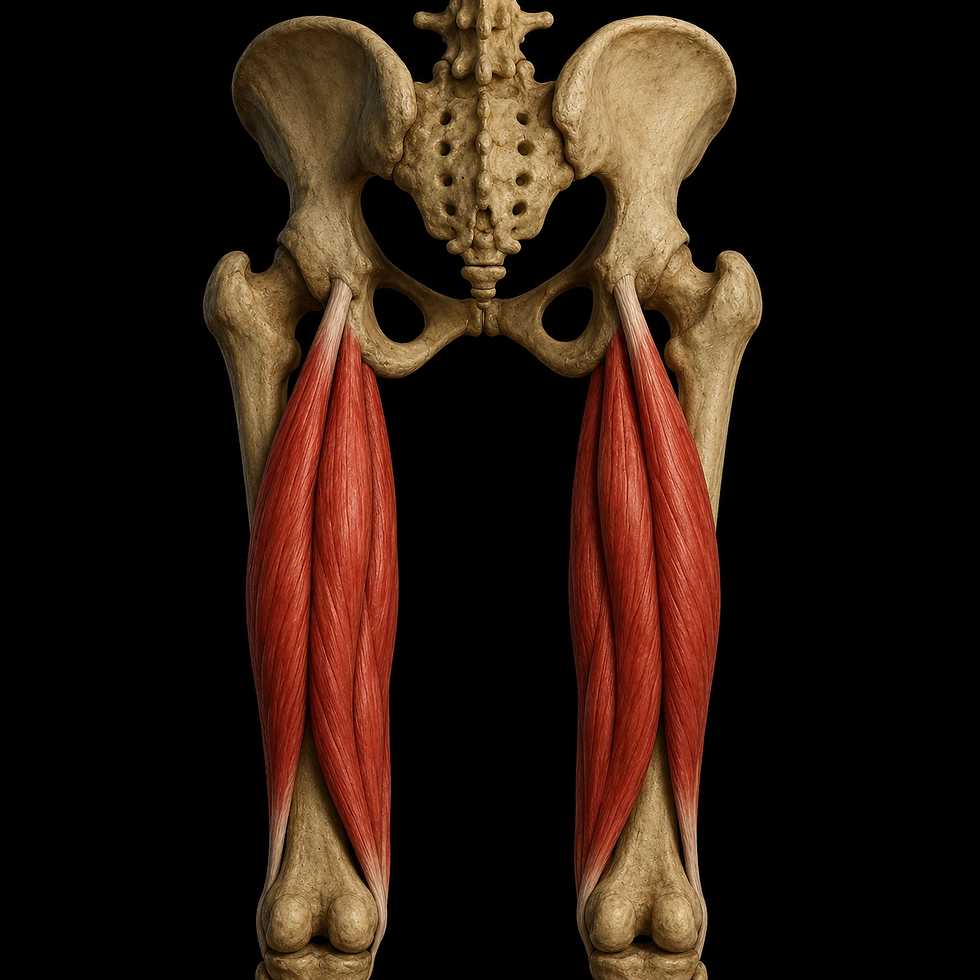
The hamstrings are a group of three long muscles located on the back of the thigh: biceps femoris, semitendinosus and semimembranosus.
Together, these muscles form most of the posterior thigh compartment and play a central role in hip extension, knee flexion, pelvic control and lower limb stability during weight bearing.
The hamstrings are especially important during walking, running, sprinting, jumping and rapid changes of direction. They help produce force, absorb load and control movement between the hip, knee and pelvis.
What makes the hamstrings particularly interesting is that most of the muscles cross two joints: both the hip joint and the knee joint. This means they influence movement and stability across a large part of the lower limb.
They also have long muscle tendon junctions, known as musculotendinous junctions. These regions extend far into the muscle tissue and are designed to tolerate high loads, transfer force efficiently and absorb mechanical stress during movement.
The Muscles of the Hamstring Group
Biceps femoris
Biceps femoris is located on the lateral side of the posterior thigh. It consists of two separate heads: a long head and a short head.
These two heads have different origins, different innervation and slightly different functional roles, but they share a common distal attachment around the lateral knee and fibular head.
The long head crosses both the hip and knee joint, while the short head only crosses the knee joint. This makes the short head functionally distinct from the rest of the hamstring group.
Semitendinosus
Semitendinosus is a long, spindle shaped muscle located on the medial side of the posterior thigh.
It lies partly superficial to semimembranosus and contributes to the pes anserinus tendon system together with sartorius and gracilis.
Because of its long tendon and medial position, semitendinosus is important for knee flexion, hip extension and medial rotation of the tibia when the knee is flexed.
Semimembranosus
Semimembranosus is the deepest and most medial muscle of the hamstring group.
It has a broad, flat proximal origin and a characteristic membranous tendon structure. This is where the muscle gets its name.
Semimembranosus has an important role in medial knee stability, hip extension and control of the posterior medial knee.
General Function
The main combined functions of the hamstrings are to flex the knee and extend the hip.
They are especially active when movement requires force, control or stability. This includes activities such as running, climbing stairs, jumping, decelerating and changing direction.
During walking, the hamstrings are active throughout parts of the gait cycle. They are particularly important at the end of the swing phase, where they slow down the forward movement of the lower leg before the foot contacts the ground.
During sprinting and explosive movement, the hamstrings work strongly as eccentric braking muscles. This means they generate force while lengthening, which helps control the limb and protect the hip and knee from excessive motion.
The hamstrings also function as dynamic stabilizers of the pelvis and lower limb. They work together with the gluteal muscles, quadriceps, adductors and calf muscles to create efficient movement throughout the entire kinetic chain.
Origin
Biceps femoris: long head
• Tuber ischiadicum
• Shares a common proximal tendon with semitendinosus
• May also have partial connection with the sacrotuberous ligament
Biceps femoris: short head
• Linea aspera
• Distal two thirds of the lateral lip
• Lateral supracondylar line of the femur
Semitendinosus
• Tuber ischiadicum
• Medial to biceps femoris
• Often originates through a common tendon with the long head of biceps femoris
Semimembranosus
• Tuber ischiadicum
• Lateral to semitendinosus
• Has a broad proximal attachment area
Insertion
Biceps femoris
• Head of the fibula
• Lateral condyle of the tibia
• Crural fascia
• Lateral intermuscular septum
Semitendinosus
• Medial surface of the tibia
• Inserts through the pes anserinus tendon system
Semimembranosus
• Posterior and medial part of the medial tibial condyle
• Broad distal tendon plate around the posterior medial knee
Innervation
The hamstrings are mainly innervated by the sciatic nerve, which is the largest peripheral nerve in the body.
The sciatic nerve consists of two main functional divisions: the tibial division and the common peroneal division. These divisions supply different parts of the hamstring group.
Semitendinosus, semimembranosus and long head of biceps femoris
• Tibial division of the sciatic nerve
• Spinal segments L5 to S2
• Provides both motor control and proprioceptive input
Short head of biceps femoris
• Common peroneal division of the sciatic nerve
• Spinal segments L5 to S2
• The only hamstring muscle that does not cross the hip joint
• Functionally and neurologically distinct from the other hamstring muscles
This innervation allows the hamstrings to react quickly and precisely during complex movement. It is especially important for coordination between the hip, knee and pelvis.
Clinical Importance of the Sciatic Nerve
The course of the sciatic nerve is clinically important because it runs close to the hamstring muscles.
Proximally, the nerve passes between the ischial tuberosity and the greater trochanter. It then travels distally along the posterior thigh, close to the hamstring muscle group.
Because of this anatomical relationship, irritation, compression, scarring or trauma near the hamstrings may contribute to radiating pain or neurological symptoms.
This may be relevant in conditions such as sciatic nerve irritation, proximal hamstring injury, deep gluteal syndrome or scar tissue after a hamstring rupture.
Blood Supply
The hamstrings have a rich blood supply from several vascular sources. This is important for muscle endurance, tissue repair and healing after injury.
Semitendinosus and semimembranosus
• Profunda femoris artery through perforating branches
• Popliteal artery
• Small branches from the inferior gluteal artery
Biceps femoris
• Profunda femoris artery through perforating branches
• Medial circumflex femoral artery
• Partial supply from the inferior gluteal artery
The venous drainage generally follows the same anatomical routes as the arterial supply.
Venous return mainly drains through the profunda femoris vein and the internal iliac venous system.
Good circulation in this region is clinically important in hamstring ruptures, tendinopathies and after surgical procedures. Blood supply affects tissue regeneration, scar formation and the overall healing process.
Anatomical and Functional Relationships
The hamstrings are located in the posterior thigh and have close relationships with surrounding muscles, connective tissue, vessels and nerves.
These relationships help explain both their function and their injury risk.
Proximally
The hamstrings originate from the ischial tuberosity.
In this region, they share anatomical connections with the proximal tendon structures of adductor magnus and parts of the gluteal region.
This makes the proximal hamstring area important for pelvic control, hip extension and force transfer between the trunk and lower limb.
Distally
The hamstrings cross the knee joint and attach either medially or laterally.
Semitendinosus and semimembranosus attach medially, while biceps femoris attaches laterally.
Together with gastrocnemius and popliteus, the hamstrings help form the posterior boundaries of the popliteal fossa.
Relationship to the sciatic nerve
The sciatic nerve runs close to the central posterior thigh.
Tightness, rupture, swelling or scar tissue in the hamstrings may therefore irritate the nerve and contribute to symptoms such as radiating pain, altered sensation or reduced neuromuscular control.
Functional Interaction With Other Muscle Groups
The hamstrings rarely work in isolation.
They are part of a larger movement system involving the pelvis, hip, knee, ankle and foot.
They work closely with several important muscle groups.
Gluteus maximus
The hamstrings cooperate with gluteus maximus during hip extension.
This is especially important during running, climbing stairs, jumping and rising from a seated position.
Quadriceps femoris
Quadriceps femoris acts as the main antagonist to the hamstrings during knee movement.
While the quadriceps extend the knee, the hamstrings flex the knee and help control anterior tibial translation during dynamic activity.
Adductor group
The adductors help stabilize the pelvis and hip.
Together with the hamstrings, they contribute to control of the femur during walking, running and single leg loading.
Triceps surae
The calf muscles contribute to propulsion during the final phase of stance.
The hamstrings coordinate with the calf complex to control the transition from hip extension to push off.
This functional interaction means that weakness, pain or injury in one part of the hamstring group can affect the entire movement chain.
A hamstring injury may therefore influence pelvic control, running mechanics, knee stability
and loading patterns through the hip, knee and ankle.
Clinical Importance and Common Injuries
The hamstring muscles are among the most frequently injured muscle groups in the body, especially in athletes involved in sprinting, football, handball, athletics and other high speed sports.
This is mainly due to the combination of high mechanical load, rapid changes in muscle length and tension, and simultaneous activation across both the hip and knee.
Hamstring injuries can range from mild overload and small muscle strains to complete ruptures or avulsions from the ischial tuberosity. The clinical presentation depends on the location, severity and mechanism of injury.
Common Types of Hamstring Injuries
Hamstring strain or rupture
Hamstring strains most often occur in the long head of biceps femoris.
This type of injury typically happens during eccentric loading, such as sprinting, sudden acceleration or rapid deceleration.
The severity can vary considerably. Mild injuries may involve small microtears in the muscle fibers, while more severe injuries may involve partial or complete muscle rupture.
Typical symptoms include sudden posterior thigh pain, reduced strength, pain during running or stretching, and sometimes bruising or swelling within the first 24 to 48 hours.
Proximal hamstring tendinopathy
Proximal hamstring tendinopathy is a chronic irritation of the tendon attachment at the ischial tuberosity.
It often develops after repeated loading in positions involving hip flexion combined with hamstring activation. This may occur during rowing, cycling, deep squats, hill running or repeated forward leaning movements.
The pain is usually deep and localized near the sitting bone. It is often provoked by prolonged sitting, running uphill, lunging or loaded hip flexion.
This condition may develop gradually and can become persistent if load management is poor.
Hamstring avulsion injury
A hamstring avulsion is a rare but serious injury where the tendon is pulled away from the ischium.
In some cases, a small bone fragment may also be pulled off with the tendon.
This injury may occur during forceful hip flexion combined with knee extension, such as during a slip, fall, high kick or sudden overstretch.
Hamstring avulsions are more common in young athletes and may require surgical assessment, especially when multiple tendons are involved or there is significant tendon retraction.
Reinjury
Hamstring injuries have a high reinjury rate.
This often happens because recovery time is underestimated, return to sport is rushed or rehabilitation is not progressed in a sufficiently structured way.
Reinjury commonly occurs in the same muscle and in the same region as the original injury.
For this reason, rehabilitation should focus not only on pain reduction, but also on strength symmetry, eccentric capacity, sprint tolerance, pelvic control and gradual exposure to sport specific demands.
Examination and Special Tests
A hamstring examination should always include a combination of history taking, palpation, movement testing, strength testing and functional assessment.
The aim is to identify the injured structure, estimate severity, detect possible neurological involvement and guide rehabilitation progression.
Palpation
Palpation should be performed along the entire length of the hamstring muscles.
The proximal tendon attachment at the ischial tuberosity should also be assessed.
In acute injuries, palpation often reveals localized tenderness, increased tissue sensitivity and sometimes a palpable defect.
Bruising or hematoma may appear within 24 to 48 hours after injury, depending on the severity and depth of the tissue damage.
Movement tests
The movement assessment should include both active and passive movement of the hip and knee.
Important tests include:
• Active hip extension
• Active knee flexion
• Passive hip flexion
• Passive knee extension
• Straight Leg Raise test
• 90/90 hamstring test
• Slump test when neurological symptoms are suspected
Reduced range of motion, pain during stretch or pain during active contraction may indicate hamstring involvement.
If symptoms include radiating pain, numbness, tingling or altered sensation, the sciatic nerve and lumbar spine should also be considered.
Special Tests
Modified Askling’s H Test
The Modified Askling’s H Test is used to assess fear, pain and readiness after hamstring injury.
The patient lies supine while the examiner rapidly lifts the leg into hip flexion with slight knee flexion.
A positive test is indicated by pain, insecurity or a clear fear of stretching in the posterior thigh.
This test is considered clinically useful after hamstring rupture because it challenges the muscle in a way that resembles the rapid stretch mechanism often involved in injury.
Isometric hamstring strength test
Isometric strength testing can be performed with a handheld dynamometer or fixed dynamometer setup.
This is useful for objective assessment after injury and during return to sport decisions.
A strength difference of more than 10 to 15 percent between sides may indicate increased risk of reinjury, especially if combined with pain, reduced sprint tolerance or poor eccentric control.
Strength should ideally be tested at different knee angles, since hamstring function changes depending on muscle length and joint position.
Functional Role in Movement and Sport
The hamstrings are not only knee flexors and hip extensors.
They are an integrated part of the entire kinetic chain and contribute to movement control from the pelvis to the foot.
Hip extension during stance phase
During walking and running, the hamstrings assist gluteus maximus in extending the hip.
This is especially important during powerful push off, acceleration and sprinting.
When the hamstrings are weak or poorly coordinated, the body may compensate through increased lumbar extension, reduced hip drive or altered stride mechanics.
Eccentric knee control during swing phase
During running, the hamstrings decelerate the forward movement of the tibia in the late swing phase.
This eccentric braking function protects the knee joint and helps control the position of the lower leg before foot contact.
This role is particularly important in sprinting, where the hamstrings must tolerate very high forces while lengthening rapidly.
Pelvic stabilization
Because the hamstrings connect the pelvis to the tibia and fibula, they play an important role in pelvic control.
They influence posterior pelvic tilt, hip position and lower limb alignment, especially during standing, bending, running and single leg loading.
Poor hamstring function may contribute to reduced pelvic control, altered lumbar loading and inefficient hip mechanics.
Synergist in hip adduction and knee control
Semimembranosus and semitendinosus work together with the adductor group in several functional movements.
This includes rising from a chair, stair climbing, cutting movements and dynamic lower limb rotation.
The medial hamstrings contribute to control of tibial rotation and medial knee stability, while biceps femoris contributes more to lateral knee control and external rotation of the tibia.
Exercises for Strengthening and Rehabilitation of the Hamstrings
The following exercises target the hamstring group through different combinations of hip extension, knee flexion, eccentric loading and pelvic control.
Variation in joint angle, load, movement speed and contraction type is important to train the full functional capacity of the hamstrings.
Exercise selection should always be adapted to the injury phase, pain level, strength capacity and functional goals.
Nordic Hamstring Exercise
Purpose
The Nordic Hamstring Exercise is primarily used for eccentric strengthening of the hamstrings.
It has documented value in reducing the risk of hamstring injuries in athletes when used consistently as part of a structured prevention program.
Execution
The person starts in a kneeling position with the feet fixed by a partner, bar or stable support.
The body is lowered slowly forward while the hips are kept extended.
The hamstrings work eccentrically to resist the forward fall.
When control is lost, the person catches themselves with the hands and pushes back to the starting position.
Effect
• Very high activation of biceps femoris
• Strong eccentric stimulus for the entire hamstring group
• Particularly useful for sprint based sports
• Can reduce hamstring injury risk when performed regularly
Recommendation
Start with 2 to 3 sets of 5 to 8 repetitions.
Perform 2 to 3 times per week in the beginning.
Progress gradually, especially if the athlete is not used to eccentric hamstring training.
Romanian Deadlift
Purpose
The Romanian Deadlift strengthens the hip extensors through both eccentric and concentric work.
It is especially useful because it trains the hamstrings at longer muscle lengths.
Execution
Stand with a barbell or dumbbells.
Keep the back neutral and the knees slightly bent.
Move the hips backward while lowering the weight along the thighs toward the mid shin.
Return to the starting position by extending the hips and keeping the spine controlled.
Effect
• Good activation of semitendinosus and semimembranosus
• Trains the hamstrings in a lengthened position
• Improves hip hinge mechanics
• May contribute to increased fascicle length over time
Recommendation
Use 3 sets of 8 to 10 repetitions.
Increase the load gradually while maintaining good control and technique.
Glute Ham Raise
Purpose
The glute ham raise combines hip extension and knee flexion.
This makes the exercise highly relevant for running, sprinting and sport specific hamstring function.
Execution
The exercise is performed in a glute ham machine or with a stable improvised setup.
Start with the hips extended and the knees flexed.
Lower the upper body under control while the knees gradually extend.
Return to the starting position by activating the hamstrings and pulling the body back up.
Effect
• High activation of biceps femoris and semitendinosus
• Trains both knee flexion and hip extension
• Useful for developing posterior chain strength
• Can support sprint performance when progressed appropriately
Recommendation
Use 2 to 3 sets of 6 to 10 repetitions.
Adjust volume and difficulty according to strength level and movement control.
Hip Thrust With Hamstring Focus
Purpose
This variation emphasizes dynamic hip extension with increased posterior chain activation.
By placing the feet slightly farther forward than in a standard hip thrust, the hamstrings are challenged more.
Execution
Place the upper back against a bench.
Position the feet farther forward than usual.
Push the hips upward while keeping control through the pelvis.
Squeeze the glutes at the top, but avoid excessive lumbar extension.
Lower back down with control.
Effect
• Activates both biceps femoris and gluteus maximus
• Trains hip extension with relatively low knee stress
• Useful in rehabilitation when knee loading must be managed
• Can be progressed with external load over time
Recommendation
Use 3 sets of 8 to 12 repetitions.
Progress with load, tempo or single leg variations when appropriate.
Slider Leg Curl
Purpose
The slider leg curl trains the hamstrings through knee flexion and eccentric control.
It is especially useful in rehabilitation because the exercise can be adjusted easily and performed with low external load.
Execution
Lie on the back with the feet placed on sliders or towels on a smooth floor.
Lift the hips from the floor.
Pull the feet toward the body while keeping the hips elevated.
Slowly slide the feet away again with control.
Effect
• Activates the hamstrings through knee flexion
• Provides eccentric loading in a controlled position
• Useful after hamstring strain or rupture
• Allows gradual progression of range and load
Recommendation
Use 2 to 3 sets of 8 to 12 repetitions.
Start with a shorter range of motion if symptoms are present.
Swiss Ball Hamstring Curl
Purpose
The Swiss ball hamstring curl increases the demand for pelvic stability, trunk control and eccentric hamstring strength.
Execution
Lie on the back with the feet placed on a Swiss ball.
Lift the hips and keep the pelvis controlled.
Roll the ball toward the body by bending the knees.
Slowly extend the knees again while maintaining hip position.
Effect
• Activates both medial and lateral hamstrings
• Improves control of the pelvis and lumbar region
• Combines strength and stability demands
• Suitable as a progression from simpler hamstring curl variations
Recommendation
Use 2 to 3 sets of 10 repetitions.
Prioritize slow tempo and stable pelvic control.
Progression and Rehabilitation Guidelines
After a hamstring injury, rehabilitation should start with controlled loading and gradually progress toward higher speed, greater range of motion and sport specific demands.
Early rehabilitation often focuses on pain free isometric activation, gentle range of motion and controlled strengthening.
As symptoms improve, eccentric exercises, hip dominant loading and longer muscle length training should be introduced.
Later phases should include running drills, acceleration, deceleration, sprint exposure and change of direction when relevant.
General progression principles:
• Start with controlled exercises in a limited range of motion
• Gradually increase range, load and movement speed
• Include both hip dominant and knee dominant hamstring exercises
• Progress eccentric loading carefully
• Add sprint specific exposure before return to high speed sport
• Monitor pain response during and after training
• Avoid sudden jumps in training volume or intensity
Return to full contact sport should only be considered when the athlete has pain free maximal strength, full range of motion and near symmetrical function compared with the uninjured side.
A common clinical target is 90 to 95 percent strength compared with the healthy side, combined with pain free sprinting, confidence and good movement quality.
Nordic hamstring training should be considered as a preventive intervention in sports with high sprint demands.
Ideally, it should be introduced at least 8 to 10 weeks before the competitive season and maintained throughout the season with an appropriate dose.
Summary
The hamstrings are a powerful and complex muscle group with essential roles in hip extension, knee flexion, pelvic control and dynamic lower limb stability.
They are highly active during walking, running, sprinting, jumping and change of direction.
Because they cross both the hip and knee, tolerate high eccentric loads and work at long muscle lengths, they are also vulnerable to strain injuries.
Clinical management of hamstring problems should include careful assessment of pain, strength, mobility, nerve involvement and functional capacity.
Effective rehabilitation should combine progressive strengthening, eccentric loading, movement control and gradual return to sport specific demands.
A well planned program can reduce reinjury risk, improve performance and restore confidence in high speed movement.
Sources:
Cael, C. (2010). Functional anatomy: Musculoskeletal anatomy, kinesiology, and palpation for manual therapists. Philadelphia, PA: Wolters Kluwer Health/Lippincott, Williams & Wilkins.
Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2014). Clinically Oriented Anatomy (7th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Netter, F. (2019). Atlas of Human Anatomy (7th ed.). Philadelphia, PA: Saunders.
Palastanga, N., & Soames, R. (2012). Anatomy and human movement: structure and function (6th ed.). Edinburgh: Churchill Livingstone.
Standring, S. (2016). Gray's Anatomy (41st ed.). Edinburgh: Elsevier Churchill Livingstone.