

Lunatum Instability
- Fysiobasen

- Dec 24, 2025
- 4 min read
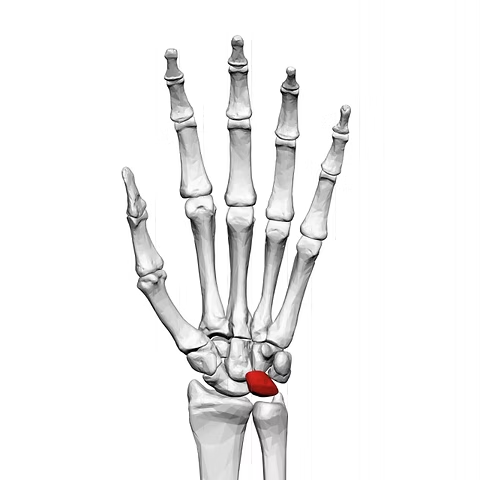
Lunatum is one of the key carpal bones of the wrist and plays a central role in maintaining stability among the carpal bones. Instability of the lunatum most often occurs due to injury to the connective tissue structures that hold the bones in place – particularly following trauma from a fall on an outstretched hand (FOOSH). If left untreated, this may lead to loss of function, degeneration, and pain during load-bearing activities¹.
Clinically Relevant Anatomy
The lunatum is located in the proximal row of carpal bones and articulates with the scaphoid, triquetrum, capitate, and hamate. It is stabilized by both intrinsic and extrinsic ligaments, including:
• Scapholunate ligament: consisting of dorsal, palmar, and proximal components
• Radioscapholunate ligament
• Dorsal intercarpal ligaments
The dorsal part of the scapholunate ligament is the thickest and most stabilizing component¹.
Mechanism of Injury
Scapholunate instability is the most common form of lunatum instability and typically occurs after a fall on an outstretched hand with the wrist in extension and ulnar deviation. The injury pattern usually starts radioulnarly and progresses to:
• Rotatory subluxation of the scaphoid
• Anterior subluxation of the lunatum• Scapholunate dissociation
• Dorsal intercalated segment instability (DISI)
• Scapholunate collapse (SLAC wrist)³
When the wrist is pronated during trauma, the lunatum may also dislocate dorsally¹.
Clinical Presentation
Patients typically report wrist pain following trauma or during load-bearing without a specific injury. Pain is usually localized between the scaphoid and lunatum and worsens with:
• Overuse activities (typing, push-ups)
• Gripping or lifting tasks
Degenerative conditions such as Madelung’s deformity, osteonecrosis, gout, or chondrocalcinosis can also lead to lunatum instability⁵.
Diagnostic Evaluation
Physical Examination
• Palpation of the scapholunate joint: directly distal to Lister’s tubercle
• Watson’s Test (Scaphoid Shift Test): positive if a “clunk” or pain reproduction occurs⁶
Imaging
• X-ray (including “clenched fist” view): may reveal the Terry Thomas sign if the gap between the scaphoid and lunatum exceeds 2 mm
• MRI/CT: indicated when assessing soft tissue and intraosseous pathology
Differential Diagnoses
Radial-sided pain:
• Carpal tunnel syndrome
• CMC1 osteoarthritis
• De Quervain’s tenosynovitis
• Scaphoid fracture
• Colles’ fracture
• C6–C7 radiculopathy
Non-specific wrist pain:
• Mechanical wrist pain (diagnosis of exclusion)
Functional Measures and Evaluation
Standardized questionnaires are valuable for assessing function and progress:
• DASH / QuickDASH
• PRWE (Patient-Rated Wrist Evaluation)
• Gartland and Werley Score
• CTQ (Brigham’s Carpal Tunnel Questionnaire)
Treatment
Conservative Management
• Immobilization with a wrist orthosis or long opponens splint
• Avoid axial loading (e.g., clenched fists)
• Distal finger block to prevent flexion under load⁸
Surgical Management
Indications:• Significant ligament injury
• Persistent instability
• Failed conservative treatment
Surgical options include:
• Ligament reconstruction (acute phase)
• Carpal fixation or arthrodesis (chronic cases)
• Tendon transposition when indicated⁴ ⁹ ¹⁰
Postoperative Follow-Up and Physiotherapy
After surgery, recommended management includes:
• Early movement of the shoulder, elbow, and fingers
• Use of a hinged wrist splint for controlled movement¹²
Progressive mobilization:– Passive → active-assisted → active free movements– Electrical stimulation may assist motor activation¹⁴
Strength and stability focus:
• Radial instability: strengthen APL, ECRL, FCR, PQ
• Ulnar instability: strengthen ECU and PQ
• Emphasis on proprioception and neuromuscular control¹⁵
Timeline:
• Week 4: gentle active exercises with protection
• Week 6–8: progression in strength and function
• After 3 months: gradual return to manual work and recreational activity
Sources:
Alonso-Tejero D, Luengo-Alonso G, Jiménez-Díaz V, García-Lamas L, Porras-Moreno MÁ, Cecilia-López D. Chronic isolated dorsal dislocation of the lunate. A rare presentation of carpal instability. Strategies in Trauma and Limb Reconstruction. 2022 Jan;17(1):59.
Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg Am. 1980;5 (3): 226-41
Kitay A, Wolfe SW. Scapholunate instability: current concepts in diagnosis and management. The Journal of hand surgery. 2012 Oct 1;37(10):2175-96.
Kitay A, Wolfe SW. Scapholunate instability: current concepts in diagnosis and management. The Journal of hand surgery. 2012 Oct 1;37(10):2175-96.
Redeker J, Vogt PM. Carpal instability. Chirurg. 2011 Jan; 82(1):85-93.
Dyer GS. Predynamic scapholunate instability. J Hand Surg Am. 2010 Nov;35(11):1879-1880.
Gjennomgått - Trukket
LaStayo P, Michlovitz S, Lee M. Wrist and Hand. In: Kolt GS, Snyder-Mackler L, eds. Physical Therapies in Sport and Exercise. 2nd ed. Philadelphia, PA: Elsevier Limited; 2007:338-346.
Wheeless C. Lunotriquetral Dissociation. Duke Orthopaedics presents Wheeless' Textbook of Orthopaedics Web site. http://www.wheelessonline.com/ortho/lunotriquetral_dissociation.
Zarkadas PC, Gropper PT, White NJ, Bertrand HP. A survey of the surgical management of acute and chronic scapholunate instability. J Hand Surg Am. 2004;29(5):848-57.
Gjennomgått - Trukket
Chinchalkar SJ, Pipicelli JG, Richards R. Controlled active mobilization after dorsal capsulodesis to correct capitolunate dissociation. J Hand Ther. 2010;23(4):404-10.
Peterson SL, Freeland AE. Scapholunate stabilization with dynamic extensor carpi radialis longus tendon transfer. J Hand Surg Am. 2010;35(A):2093-2100.
Agrawal CS, Deshmukh M, Padmawar S. Rehabilitation Protocol for Lunate Fracture in a Clinical Case Report. Cureus. 2024 Jun 7;16(6).
Cheuquelaf-Galaz C, Antúnez-Riveros MA, Lastra-Millán A, Canals A, Aguilera-Godoy A, Núñez-Cortés R. Exercise-based intervention as a nonsurgical treatment for patients with carpal instability: A case series. Journal of Hand Therapy. 2024 Jul 1;37(3):397-404.



