Psoas Major
- Fysiobasen

- Jan 11
- 11 min read
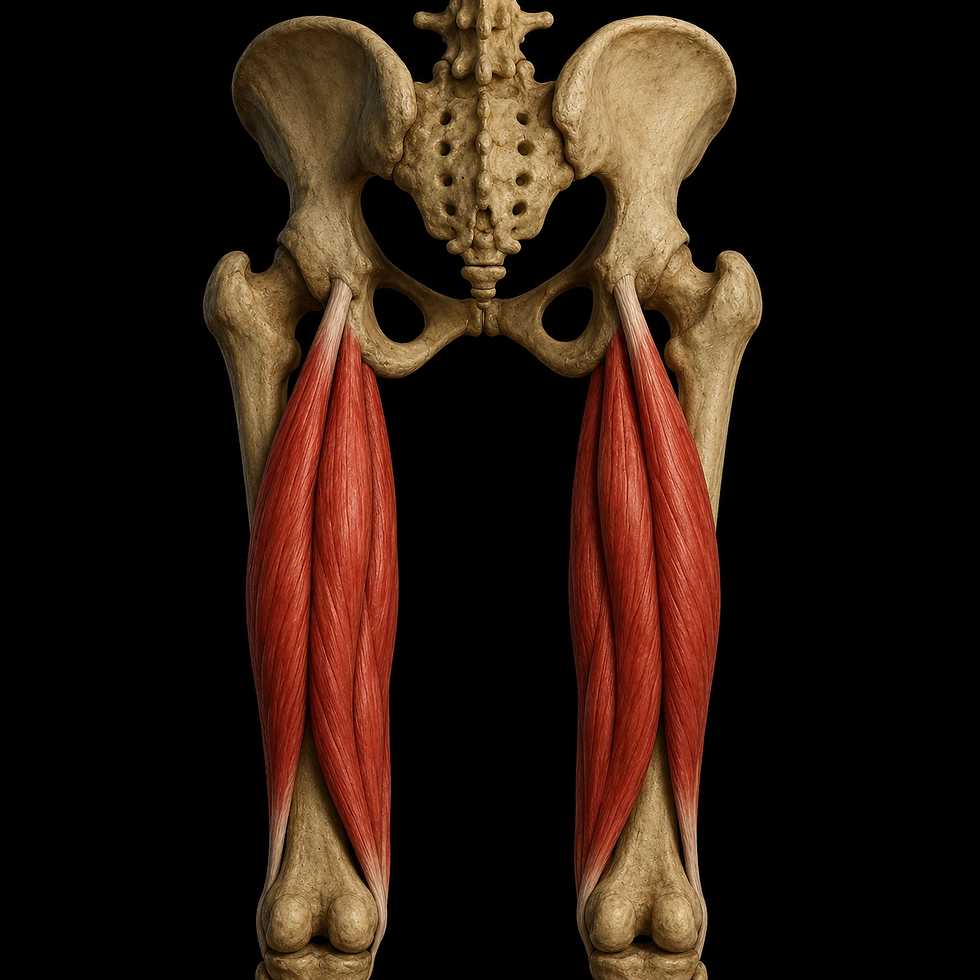
Psoas major is a long, fusiform muscle located deep within the abdomen and pelvis, functioning as a biomechanical bridge between the vertebral column and the lower extremity. Its position, structure, and multi-joint function make it central to mobility, stability, and postural control. Due to its anatomical location, psoas major is also in close proximity to visceral and neurovascular structures, giving it a level of complexity that is uncommon among skeletal muscles.

The muscle lies retroperitoneally, medial to quadratus lumborum and lateral to the vertebral column. It extends from the thoracolumbar spine to the femur and functionally belongs to the hip flexor group. As the name indicates, it is the larger of the two psoas muscles and is most commonly described together with iliacus as the iliopsoas.
Origin
Psoas major has a broad and deep origin that includes both anterior and lateral spinal structures. The origin can be divided into two anatomical components: a superficial and a deep part.
Superficial part: Arises from the lateral surfaces of the vertebral bodies of T12 to L4, as well as the corresponding intervertebral discs.
Deep part: Arises from the transverse processes of L1 to L5.
Several muscle fibers wrap around the transverse processes and share small fascial connections with quadratus lumborum. Clinically, this creates a functional interdependence between the two muscles, particularly in lateral flexion and postural control.
Between these two layers pass components of the lumbar plexus, creating a close structural relationship between muscle tissue and neural elements. Changes in muscle tone, hypertrophy, or inflammation can therefore lead to nerve compression or irritation, which is clinically relevant in conditions such as anterior lumbar radiculopathy or psoas abscess.
Transition to Insertion
After passing beneath the inguinal ligament and entering the anterior thigh region, the muscle fibers converge into a common tendon together with iliacus. This tendon, commonly referred to as the iliopsoas tendon, passes anterior to the hip joint capsule and continues toward the femur.
The tendon inserts on the lesser trochanter of the femur, a small medial bony prominence located posteroinferior to the center of the hip joint. The tendon glides over the anterior aspect of the hip capsule and does not directly contact the acetabulum, being separated instead by a large, pressure-absorbing synovial structure: the iliopectineal bursa.
This bursa reduces friction between the deep surface of the tendon and the underlying bone. It is one of the largest bursae in the body and may become irritated under conditions of high load, overuse, or compression, presenting clinically with anterior hip pain, and in some cases palpable swelling or snapping sensations in the groin.
Course Through the Abdomen and Pelvis
From its origin, the muscle fibers converge and descend inferolaterally through the pelvic cavity. The muscle follows the inner border of the pelvic ring (linea terminalis) and runs along the medial margin of the iliac fossa, parallel to the ureter and gonadal vessels. As it approaches the inguinal ligament, it begins to merge with iliacus. Together, they form a unified muscle mass that passes beneath the ligament and enters the femoral triangle.
Along its course, psoas major forms a boundary between the posterior abdominal wall and the thigh region. Anterior to the muscle lie the kidneys, ureter, and major vessels, while its posterior surface is in contact with the vertebral column and intervertebral joints.
Structural Fusion With Iliacus
Iliacus originates from the iliac fossa and converges with psoas major just proximal to the passage beneath the inguinal ligament. Although the two muscles have distinct anatomical origins, they function as a single unit during movement. Their fusion occurs within the pelvic region, making complete clinical separation of their functions impossible.
This fusion significantly increases force production during hip flexion compared to either muscle acting alone. The shared tendon is exceptionally strong and represents the body’s primary hip flexor, particularly in sitting positions and during the initial phase of gait.
Psoas major and iliacus lie on either side of the femoral nerve as they enter the femoral triangle. Both structures are located deep to the fascia lata, sartorius, and rectus femoris. The femoral nerve lies lateral to the iliopsoas tendon, while the femoral vein lies medially. Consequently, marked hypertrophy, trauma, or rupture of the iliopsoas can lead to compression of both neural and venous structures, potentially resulting in numbness, pain, or distal circulatory changes in the lower limb.
Anatomical Relationships
Psoas major is a deep retroperitoneal muscle with close relationships to multiple neurovascular, visceral, and skeletal structures within the abdomen and pelvis. These relationships are clinically significant in the assessment of referred pain, compression syndromes, and postoperative complications.
Within the abdomen, psoas major lies:
Anterior to the lumbar spine, covering the lateral aspects of the vertebral bodies and intervertebral discs from T12 to L5.
Medial to quadratus lumborum, an important relational muscle in lateral flexion.
Posteriorly in contact with the posterior elements of the lumbar vertebrae, particularly the transverse processes.
Medial relationships
The abdominal aorta runs medial and anterior to the left psoas major, while the inferior vena cava does the same relative to the right psoas major.
The sympathetic trunk lies closely medial to the muscle and may be affected by inflammation or increased muscle tone.
Lumbar lymph nodes and the cisterna chyli are also closely related.
Lateral and dorsolateral relationships
Quadratus lumborum lies directly lateral to psoas major in the upper portion of its course.
The kidneys rest on psoas major, particularly at the lower renal pole, giving the muscle relevance in renal pain and retroperitoneal surgical approaches.
The ureter crosses psoas major en route to the bladder, meaning pathological muscle activity may contribute to ureteral compression or referred flank pain.
Nerve Relationships and the Lumbar Plexus
The lumbar plexus forms within psoas major, where the anterior rami of spinal nerves L1 to L4 pass through or between the deep and superficial muscle fibers.
Femoral nerve (L2–L4): Emerges laterally between psoas major and iliacus and enters the femoral triangle.
Obturator nerve (L2–L4): Passes inferomedially through the pelvis toward the obturator foramen, exiting the muscle medially.
Genitofemoral nerve (L1–L2): Pierces psoas major and runs anteriorly on its surface before dividing.
Lateral femoral cutaneous nerve (L2–L3), iliohypogastric and ilioinguinal nerves (L1): Related to the upper lateral portion of the muscle.
This configuration makes psoas major one of the few muscles in which nerves are formed within the muscle itself. As a result, hypertrophy, inflammation, hematoma, or abscess can
easily affect neural structures, leading to motor deficits, paresthesia, or referred pain.
Pelvic and Femoral Triangle Relationships
As psoas major exits the abdomen beneath the inguinal ligament, it forms part of the floor of the femoral triangle together with iliacus.
In this region:
The tendon lies deep to the femoral artery, femoral vein, and femoral nerve.
Medial to the tendon lies the femoral vein, and lateral to it lies the femoral nerve.
The iliopectineal bursa lies between the tendon and the hip joint capsule, reducing friction.
Inflammation of the bursa, hematoma formation, or tumor development in the iliopsoas region can lead to compression of vascular or neural structures within the femoral triangle, resulting in groin pain, thigh paresthesia, or vascular compromise.
Innervation
Psoas major is innervated by the ventral rami of spinal nerves L1 to L3, with some sources also including L4. These nerves contribute to the lumbar plexus and enter the muscle directly after exiting the intervertebral foramina.
This innervation pattern makes psoas major particularly sensitive to both central and peripheral neurological influences, especially in cases such as:
Lumbar disc herniation at L2–L3, potentially causing hip flexion weakness.
Nerve root involvement, leading to reduced psoas function and pain during gait initiation or trunk flexion.
The psoas reflex, which can be assessed clinically during resisted hip flexion as part of neurological examination.
Blood Supply
Psoas major has a complex arterial supply. The primary source is:
Lumbar branch from the iliolumbar artery, originating from the internal iliac artery.
Additional contributing vessels include:
Lumbar arteries (L1–L4) from the abdominal aorta
Muscular branches from the deep circumflex iliac artery
Small branches from the femoral artery and common iliac artery in the distal portion
In some cases, contributions from renal and gonadal arteries, due to the close anatomical relationship of psoas major to these vessels
Venous Drainage
Venous drainage follows the arterial pathways and drains into:
External and internal iliac veins
Femoral vein
Inferior vena cava
Large hematomas following trauma or surgery in this region may lead to blood accumulation between the muscle and the peritoneum or within fascial planes, potentially causing significant compression and requiring urgent intervention.
Functional Anatomy and Biomechanics
Psoas major is one of the body’s most important and biomechanically complex deep muscles. Its function varies considerably depending on movement direction, body position, and coordination with surrounding muscle groups.
In open-chain conditions, where the lower limb moves freely while the trunk is stabilized, psoas major primarily functions as a hip flexor. It draws the femur forward and upward during activities such as walking, running, stair climbing, and kicking. Due to its oblique and vertical fiber orientation, it may also contribute to slight external rotation of the hip, particularly in the early phase of hip flexion.
When psoas major and iliacus activate simultaneously, forming the iliopsoas, force production is markedly increased. Iliacus has a larger physiological cross-sectional area, whereas psoas major has a longer moment arm and operates through a greater range of motion. During powerful hip flexion, such as sprint starts or high knee lifts, psoas major is the dominant muscle in the initial phase.
In closed-chain conditions, where the limb is fixed and the trunk moves, psoas major functions as a trunk flexor and lateral stabilizer. Bilateral activation contributes to lumbar flexion and anterior pelvic tilt. Unilateral activation promotes lateral trunk flexion, allowing compensation for reduced control in quadratus lumborum or the multifidus muscles.
Psoas major also plays a role in the deep lumbar stabilization system. Together with transversus abdominis, multifidus, and the diaphragm, it contributes to maintaining intra-abdominal pressure and spinal stability during loading. This is particularly important during lifting, rotational movements, and static postures requiring precise balance between mobility and control.
Clinical Significance and Load-Related Pathology
Psoas major is frequently involved in pain syndromes and functional impairments, particularly in the lower back, pelvis, and hip region. Due to its deep location, close proximity to neural and vascular structures, and biomechanical role, clinical assessment is often challenging.
One of the most recognized conditions is psoas syndrome, characterized by increased muscle tone or adaptive shortening. This may result in lumbar hyperextension, anterior pelvic rotation, and asymmetrical posture. Typical symptoms include unilateral low back pain, reduced hip extension, and referred pain to the groin or anterior thigh. Symptoms often worsen in supine positions with the hip extended or during lunging movements.
Prolonged inactivity, such as sustained sitting, leads to adaptive shortening of psoas major. This alters pelvic alignment, increases hip flexor tightness, and may inhibit gluteal musculature, particularly gluteus maximus. The resulting imbalance increases strain on the lumbar extensors and disrupts movement efficiency.
Trauma, surgery, or infection may result in a psoas abscess, a rare but serious condition presenting with pain, fever, tenderness, and possible compression of lumbar nerves or the ureter. This typically requires imaging and drainage. Similarly, postoperative bleeding or hematoma formation in the psoas region can restrict hip motion, cause paresthesia, and impair gait.
Rehabilitation, Treatment, and Training
Physiotherapeutic management of psoas-related dysfunction requires comprehensive functional analysis, including assessment of muscle length, tone, activation patterns, and relationships with core stability and hip control.
In cases of tight or overactive psoas, treatment often combines manual therapy, stretching, and neuromuscular retraining. Common stretches include lunges with the trailing leg in extension, active hip extension in side-lying, and modified Thomas stretching. Simultaneous activation of antagonists, particularly gluteus maximus and the hamstrings, is essential for lasting changes in length–tension relationships.
In cases of weak or hypoactive psoas major, such as post-surgical or neurological involvement, rehabilitation focuses on isolated activation in controlled movement patterns. Exercises may include seated resisted hip flexion, supported straight-leg raises in supine, or standing knee lifts on unstable surfaces.
Functional rehabilitation emphasizes integrated movement patterns where psoas activation occurs as part of coordinated tasks. Examples include diagonal knee lifts with trunk rotation, balance lunges, and running-specific drills targeting hip and core strength.
Advanced rehabilitation should include assessment of rotational strength and frontal-plane stability, as psoas major is active across multiple planes during dynamic movement. Breathing patterns and diaphragmatic control should also be evaluated, given the fascial and functional relationship between the diaphragm and psoas in deep stabilization.
Neurological and Orthopedic Differential Diagnosis
Psoas-related pain may be misinterpreted as groin pathology, iliacus dysfunction, iliopsoas bursitis, lumbar radiculopathy, or sacroiliac joint disorders. The following assessments should therefore be considered:
Straight leg raise and slump tests for radicular involvement
Thomas test for hip flexor contracture
Deep abdominal palpation of psoas major
Evaluation of postural alignment and gait mechanics
Exercises for Psoas Major: Activation, Mobility, and Functional Control
1. Supine Active Isolated Hip Flexion
Purpose: Isolated activation of psoas major with minimal compensation from rectus femoris and abdominal muscles.
Execution: The patient lies supine with one leg extended and the other flexed with the foot on the floor. The extended leg is slowly lifted to approximately 30–40 degrees of hip flexion without knee flexion. The lumbar spine remains neutral, avoiding anterior pelvic tilt. Hold for 2 seconds and lower under control.
Progression: Add ankle weights, elastic resistance, or bilateral leg lifts with strict lumbar control.
Clinical relevance: Suitable for patients with reduced isolated psoas activation following surgery or neuromuscular inhibition.
2. Dynamic Thomas Stretch With Activation
Purpose: Lengthening and mobilization of a shortened psoas major with simultaneous neuromuscular recruitment.
Execution: The patient lies on a bench with one hip off the edge while the opposite knee is held toward the chest. The hanging leg is allowed to descend passively under gravity. The gluteal muscles are then activated to enhance the stretch. Hold for 30 seconds, repeat 3–5 times.
Variation: Actively lift the hanging leg a few centimeters before slowly lowering it to add eccentric control.
Clinical relevance: Highly effective for anterior pelvic tilt and lumbar hyperextension associated with psoas tightness.
3. Standing Resisted Knee Lift
Purpose: Functional strengthening of psoas major in a closed-chain position with controlled hip flexion.
Execution: The patient stands upright with resistance band anchored behind and looped around the ankle. The knee is lifted to hip height against resistance while maintaining upright posture and smooth movement. Controlled return to start.
Progression: Perform on a balance surface or in a split-stance position for increased control demands.
Clinical relevance: Transfers well to gait and sport-related activities, with strong activation of psoas and core musculature.
4. Dead Bug With Hip Flexion Emphasis
Purpose: Coordinated control between psoas major and deep abdominal muscles.
Execution: The patient lies supine with hips and knees at 90 degrees. One foot lowers toward the floor while the opposite leg remains stable. The lumbar spine stays pressed into the surface without spinal movement.
Progression: Add resistance bands between the knees or ankle weights, or combine with arm movements.
Clinical relevance: Reduces compensation from rectus femoris and promotes selective psoas activation with core engagement.
5. Modified Lunge With Psoas Stretch and Activation
Purpose: Combine active stretching of the trailing-leg psoas with controlled activation in the lead leg.
Execution: The patient performs a deep lunge with the rear leg supported on a bench. Posterior pelvic tilt increases the psoas stretch. The rear gluteal muscles are activated to stabilize the pelvis, while the front leg performs small controlled lunges.
Progression: Add trunk rotation toward the front leg to increase fascial and neuromuscular demand.
Clinical relevance: Effective for limited hip extension and impaired lumbopelvic control.
6. Marching With Resistance
Purpose: Build strength and endurance of psoas major in a weight-bearing, functional position.
Execution: The patient walks forward while lifting each knee to hip height with controlled lowering. Resistance may be added via weight vest, dumbbells, or elastic bands. Maintain upright posture and rhythmic activation.
Clinical relevance: Highly transferable to walking, stair climbing, sprinting, and transitional movements.
Sources:
Drake, R., A.W. Vogl, A.W., Mitchell, A.W. M. (2015). Gray’s Anatomy for Students, 3rd Edition, Churchill Livingston Elsevier
Moore, K.L., Agur, A.M.R., Dalley, A.F. (2015). Essential Clinical Anatomy, 5th Edition, Wolters Kluwer
Netter, F. (2014). Atlas of Human Anatomy, 6th Edition, Elsevier Saunders
Psoas Syndrome Management and Treatment | Cleveland Clinic. (2019). Retrieved 14 November 2019, from https://my.clevelandclinic.org/health/diseases/15721-psoas-syndrome/management-and-treatment
Standring, S. (2008). Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 14th Edition, Churchill Livingston Elsevier
Tufo, A., Desai, G.J., Cox, W.J. (2012) Psoas Syndrome: A Frequently Missed Diagnosis, The Journal of the American Osteopathic Association, Vol.112, p.522-528.