Quadratus Lumborum
- Fysiobasen

- Jan 11
- 9 min read
The quadratus lumborum is a deep posterior trunk muscle located in the lumbar region and forms a central component of the posterior abdominal wall. It has a rectangular shape, and its name literally means “square lumbar muscle.” It plays a key role in stabilisation of the lumbar spine and in the thoracic breathing pattern, and is frequently involved in lumbar pain conditions—both as a primary pain source and as a compensatory muscle.
Origin
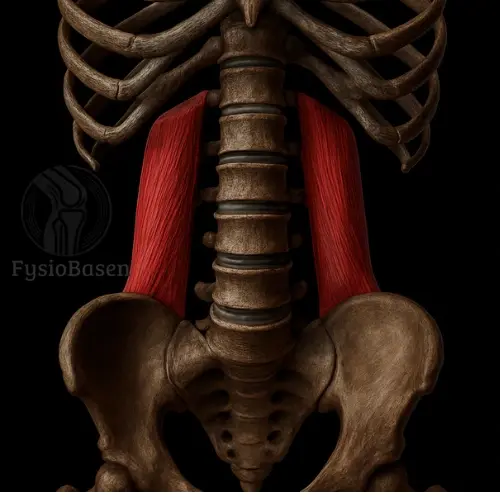
The quadratus lumborum originates from the iliac crest (posterior portion of the iliac crest) and the iliolumbar ligament.
In addition, some fibres originate from the aponeurosis of the transversus abdominis.
This provides the muscle with a robust and stable pelvic attachment, making it well suited to act as a “bridge” between the pelvis and the spine.
Insertion
The muscle inserts on the inferior border of the 12th rib and on the transverse processes of L1–L4.
These attachments allow the muscle both to elevate the pelvis and to draw the rib cage downward, supporting important functions in posture and respiration.
Location and Layering
The quadratus lumborum lies deep within the posterior abdominal wall, directly anterior to the erector spinae muscles and posterior to the kidneys. It is enclosed by the thoracolumbar fascia, which both protects the muscle and provides structural support in coordination with the abdominal musculature.
Laterally, it borders the transversus abdominis, while medially it lies in close proximity to the lumbar spine. Anteriorly, it relates to the kidneys and the psoas major, making the quadratus lumborum clinically relevant in both lumbar and abdominal conditions.
Due to its deep location, palpation is challenging but possible during side bending and light activation, palpating beneath the rib cage and above the iliac crest.
Relationship to the Diaphragm and Breathing
The quadratus lumborum has close anatomical and functional relationships with the diaphragm. It contributes to stabilisation of the 12th rib and prevents it from being pulled cranially during inspiration. In this way, the quadratus lumborum indirectly provides a fixed anchor point for effective diaphragmatic contraction, which is particularly important during physical activity or in individuals with reduced lung capacity.
During inspiration with a fixed pelvis, the quadratus lumborum may assist in depressing the 12th rib and increasing thoracic volume. As a result, it often compensates in cases of reduced diaphragmatic function.
Clinical Observations and Activation Patterns
The quadratus lumborum is well known for its role in hip hitching, i.e. elevation of the pelvis on one side—a compensatory movement frequently observed in leg length discrepancy or limping following injury. Unilateral activation produces lateral flexion of the spine, whereas bilateral activation results in stabilisation and slight extension.
Clinicians often observe increased tone and referred pain from the quadratus lumborum in association with:
Prolonged standing work
Asymmetrical loading of the spine or pelvis
Respiratory dysfunction, where the quadratus lumborum overactivates to assist the diaphragm
Gait patterns with asymmetrical pelvic motion
Function
The quadratus lumborum acts primarily in two ways, depending on whether the pelvis or the rib cage is fixed.
With the Thorax Fixed
Elevates the pelvis on the ipsilateral side (hip hitching).
Important during gait, particularly when the contralateral hip flexors swing the leg forward.
With the Pelvis Fixed
Draws the 12th rib downward and posteriorly, supporting diaphragmatic function during forceful inspiration.
Produces lateral flexion of the spine during unilateral contraction.
During bilateral contraction, contributes to extension and stabilisation of the lumbar spine.
Stabilising Function
Works closely with the deep abdominal muscles (particularly the transversus abdominis) and the multifidus muscles to create lumbar stability, both statically and dynamically.
Is reflexively activated during balance challenges and rotational forces acting on the trunk.
Innervation
The quadratus lumborum receives its nerve supply from the lumbar plexus, specifically:
Subcostal nerve (T12)
Iliohypogastric nerve (L1)
Ilioinguinal nerve (L1)
Segmental branches from L1–L3
These nerves provide motor innervation and are clinically important when assessing neurological function in the region. The nerve roots course in close proximity to the muscle, making the quadratus lumborum sensitive to neurogenic irritation or reflex muscle tension.
Blood Supply
The quadratus lumborum is supplied by several small arterial branches, making it relatively resistant to ischaemic injury:
Lumbar arteries (from the abdominal aorta)
Iliolumbar artery (from the internal iliac artery)
Small branches from the subcostal artery and 11th–12th intercostal arteries
This rich blood supply supports high metabolic activity and underpins the muscle’s ability to sustain prolonged postural loading.
Clinical Significance
The quadratus lumborum is a frequent source of myofascial pain, and trigger points commonly refer pain to:
The lateral iliac crest
The sacroiliac joint
The lower abdomen
The lower thoracic spine
The upper gluteal region
Common Clinical Presentations
Unilateral low back pain without nerve root involvement
Pain during side bending to the contralateral side
Symptom aggravation after prolonged static standing
Pain during breathing, coughing, or laughter when the muscle is hypertonic
Functional Consequences of Quadratus Lumborum Dysfunction
Compensatory gait patterns with lateral trunk sway
Pelvic asymmetry
Increased compressive load on the lumbar spine
Altered breathing patterns, particularly with reduced diaphragmatic contribution
Examination and Palpation
Palpation of the quadratus lumborum is technically demanding and requires clinical experience. The patient is positioned in side-lying or prone. The examiner palpates deeply between the iliac crest and the 12th rib, directing pressure toward the posterior abdominal wall. The lateral and inferior fibres are most accessible.
Muscle tightness may be assessed during side bending, as well as with functional tests such as a modified Thomas test or active hip hitching.
Palpation and Clinical Examination
Palpation of the quadratus lumborum (QL) requires experience and precision due to its deep location behind the abdominal viscera and anterior to the more superficial spinal extensors.
Patient Positioning
Side-lying with slight flexion of the hip and knee
The spine should be gently flexed to expose the contour of the lateral lumbar region
Alternatively, prone positioning with support under the abdomen to reduce lumbar lordosis
Palpation Technique
Place the fingers directly above the iliac crest and move cranially toward the 12th rib
Apply gentle but deep pressure laterally into the abdomen, just lateral to the erector spinae
Ask the patient to lift the pelvis or perform a light upward pull; the QL will then contract and become more prominent
Assess for tightness, tenderness, and side-to-side differences in muscle tone
Signs of QL Dysfunction on Palpation
Palpable tenderness at the origin or insertion
Distinct deep trigger points (often 2–3 primary points)
Referred pain upon pressure (e.g. to the gluteal region, groin, or sacroiliac joint)
Unilateral hypertonicity and muscle shortening
Differential Diagnosis
Pain originating from the quadratus lumborum may mimic several other conditions. It is therefore essential to distinguish between muscular, neurogenic, and visceral causes of lumbar and pelvic pain.
Differential Diagnoses to Consider
Lumbar radiculopathy→ Radiating pain below the knee and positive neurological tests
Sacroiliac joint dysfunction→ Posterior and inferior pain with positive provocation tests
Psoas major tightness→ More medial pain, reduced hip extension, positive Thomas test
Lumbar facet joint pathology→ Pain provoked by rotation and extension, localised to the lumbar spine
Nephritis or renal calculi→ Deep flank pain, haematuria, fever, no muscular tenderness on palpation
Appendicitis or retrocaecal inflammation→ Right-sided abdominal pain that may mimic QL pathology
When in doubt, organic pathology must always be excluded before diagnosing a musculoskeletal condition.
Physiotherapeutic Treatment and Activation
Treatment of QL dysfunction should always be part of a comprehensive assessment of the pelvis, hip, and lumbar spine. Interventions should be directed toward:
Relaxation in cases of hyperactivity
Strengthening in cases of instability
Mobility in cases of unilateral shortening
Passive Interventions for Pain or Tightness
Myofascial release and trigger point therapy
Needling techniques (IMS or dry needling) for deep trigger points
Heat therapy to promote muscle relaxation
Mobilisation of the thoracolumbar junction
Diaphragm-focused breathing for indirect relaxation (QL often overactivates during dysfunctional breathing)
Active Exercises for Strength and Control
Side-lying hip hitching→ The patient lies on the side and lifts the upper pelvis without using the leg muscles→ Emphasis on control and isolation
Bird dog with rotation and side-bending→ Increased QL activation when the arm and leg are lifted and the trunk is rotated→ Controlled execution with focus on lumbar stability
Standing hip hike on a box→ Standing with one foot on a box, lifting the opposite side of the pelvis→ Promotes functional QL activation
Side plank with pelvic lift→ Static and dynamic control with high load on the ipsilateral QL
“Bamboo exercise” (dynamic side bending)→ Use of a barbell or dowel to actively bend side to side→ Effective for mobility and control of the lateral bending axis
Rehabilitation Principles
Rehabilitation of the quadratus lumborum should include:
Restoration of symmetry between the right and left sides
Integration of QL training with breathing techniques and pelvic control
Addressing underlying factors such as leg length discrepancy or hip dysfunction
Combining strengthening and stretching for balanced muscle use
Early inclusion of functional exercises to prevent compensatory patterns
In long-standing QL dysfunction, symptoms may become self-perpetuating through compensatory movement patterns. Breaking this cycle requires specific and patient guidance.
Exercises for the Quadratus Lumborum
The quadratus lumborum primarily acts as a lateral stabiliser of the lumbar spine and plays a key role in side bending, pelvic elevation, postural control, and diaphragmatic stabilisation. It is most active when the body must control lateral forces or compensate for instability in the pelvis and lumbar spine.
Exercise selection should be based on:
The need for strength, control, or relaxation
Unilateral versus bilateral function
Whether the QL acts as a prime mover or a stabiliser
1. Side-Lying Hip Hitching
Purpose: Isolated activation of the ipsilateral QL in a shortened position
Execution:
The patient lies on the side with hips and knees slightly flexed
The upper leg remains relaxed; the pelvis is lifted toward the ribs
Hold for 3–5 seconds, then return slowly
Focus: The QL shortens and activates concentrically. Ensure the patient does not compensate with the gluteal or hamstring muscles.
Evidence: EMG studies demonstrate high QL activation in this position, especially when performed slowly with isolated movement (McGill et al., 2009).
2. Side Plank With Hip Lift
Purpose: Increase QL strength and endurance as part of core stability
Execution:
Standard side plank from knees or feet
The pelvis is lowered in a controlled manner and lifted back to neutral
Can be progressed using resistance bands
Focus: The QL works eccentrically and concentrically during pelvic lowering and lifting. High neuromuscular control is required.
Evidence: Several studies (e.g. Ekstrom et al., 2007) show that dynamic side plank variations elicit higher activation than static holds, with particularly high QL activity during lateral instability.
3. Bird Dog With Lateral Flexion
Purpose: Dynamic control and integration with the spinal extensors
Execution:
From quadruped, lift the opposite arm and leg
Bring elbow and knee toward each other with diagonal rotation
Add a gentle lateral flexion before returning to neutral
Focus: The QL activates to prevent collapse of the lumbar spine, challenging both stability and coordination.
Evidence: This variation produces higher QL activation than the standard bird dog, particularly on the weight-bearing side (Borghuis et al., 2008).
4. Standing Hip Hike on a Step
Purpose: Functional QL strength and control in a weight-bearing position
Execution:
Stand with one foot on a step, the other hanging freely
Lift the hanging side by elevating the pelvis
Hold for 2 seconds, then lower slowly
Focus: Isolates the QL responsible for elevating the pelvis on the unsupported side. Also activates the gluteus medius and lateral core musculature.
Evidence: Commonly used in rehabilitation of pelvic instability and low back pain (Richardson & Jull, 1995), providing high QL activation without excessive spinal load.
5. Side-Lying Leg Raise With Rotation
Purpose: Combined activation of the QL and oblique abdominal muscles
Execution:
The patient lies on the side with the forearm supporting the upper body
Lift the upper leg while simultaneously rotating the trunk backward
Perform slowly and with control in both directions
Focus: Creates transverse loading of the QL through combined side bending and rotation.
Evidence: Lower load than side planks but suitable early in rehabilitation. EMG analyses show activation of both the QL and internal oblique muscles (Cresswell et al., 1994).
6. Resistance Breathing (QL–Diaphragm Interaction)
Purpose: Indirect QL activation through deep core and respiratory muscles
Execution:
The patient lies supine with knees bent
Performs slow, controlled breathing against resistance (e.g. PEP device or pursed-lip breathing)
Focus on expanding the lateral rib cage and creating pressure into the flanks
Focus: Enhances coordination between the QL and diaphragm, particularly important in chronic low back pain.
Evidence: Widely used in respiratory physiotherapy and lumbar instability rehabilitation; shown to reduce QL hyperactivity (Hodges et al., 2005).
How to Choose the Appropriate Exercise
Selection should be based on:
Relaxation: breathing, massage, mobilisation
Early activation: side-lying hitch, bird dog
Strength: hip hike, side plank
Functional integration: standing rotations, asymmetrical carrying
Endurance: prolonged side plank holds, breathing control
All exercises should be supervised by a physiotherapist and adjusted to the individual’s functional level. For optimal outcomes, the quadratus lumborum should never be trained in isolation over time but integrated with pelvic control, thoracolumbar mechanics, and hip stability.
References
Drenckhahn, D., & Waschke, J. (2008). Taschenbuch Anatomie (1st ed.). Urban & Fischer / Elsevier.
Schünke, M., Schulte, E., & Schumacher, U. (2007). Prometheus – Atlas of Anatomy: General Anatomy and Musculoskeletal System (2nd ed.). Thieme.
Fors, S. (2007). Why We Hurt – A Complete Physical and Spiritual Guide to Healing Your Chronic Pain. Llewellyn Publications.
Cael, C. (2010). Functional Anatomy: Musculoskeletal Anatomy, Kinesiology, and Palpation for Manual Therapists. Wolters Kluwer.
Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2014). Clinically Oriented Anatomy (7th ed.). Lippincott Williams & Wilkins.
Netter, F. (2019). Atlas of Human Anatomy (7th ed.). Saunders.
Palastanga, N., & Soames, R. (2012). Anatomy and Human Movement (6th ed.). Churchill Livingstone.
Standring, S. (2016). Gray’s Anatomy (41st ed.). Elsevier Churchill Livingstone.